Two years and more than a million prescriptions after Wegovy first went on sale, there’s one taboo question for some doctors who prescribe the hit obesity drug: When can patients stop taking it?
The new medicine by Novo Nordisk A/S and others in the same class can melt away pounds that diet and exercise don’t budge. But it doesn’t change the underlying issues that drive metabolism, leaving newly lean people wondering whether they will need to bear the expense and the side effects of the drugs for decades or risk relapse.
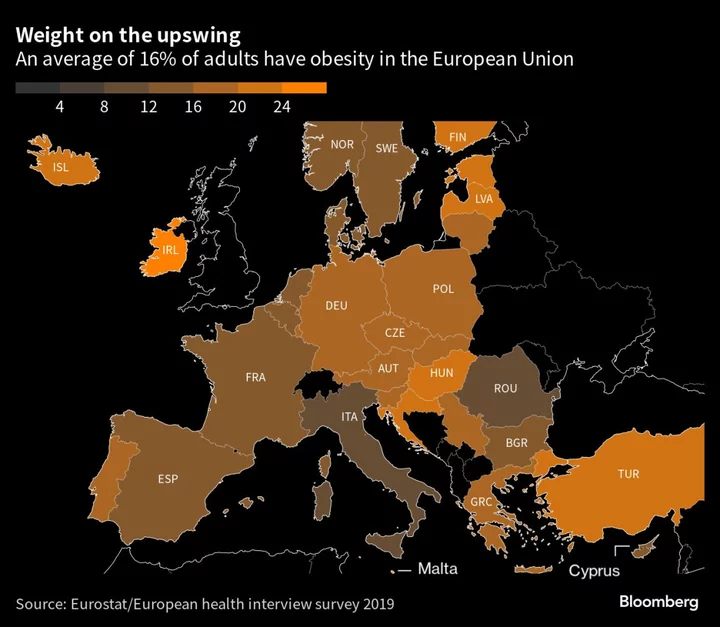
The weight rebound is a growing problem in the US as some insurers balk at the drug’s more than $1,000-a-month price, a situation that will be more acute in Europe’s cash-strapped public health-care systems. A UK health agency has already recommended capping care at two years. At stake are billions of dollars and a fundamental issue: whether obesity should be treated as a disease long after its most visible symptom has vanished.
“The question that’s out there is, do you do this forever?” said Ethan Balk, a clinical dietitian with Yale New Haven Health’s Center for Weight Management. He believes people should accept that weight management in some form is a “forever thing,” just like overseeing one’s finances or schedule.
Reluctant insurers in the US have made the new category of weight-loss medicines a pay-as-you-go proposition for most patients, and the expense alone is pushing some off the treatment. In Europe, where Wegovy’s rollout in major markets is set to start next month, prices will be lower, but many patients will probably need to pay out of pocket and only take the drug as long as they can afford it. In Norway and Denmark, where Wegovy is already on sale, one month’s supply costs about $350 at most.
The new class of drugs mimics a hormone that curbs appetite, turning people off food. But when they stop treatment, the pounds tend to return in a yo-yo pattern familiar to almost anyone who’s dieted.
“The body fights back,” says Gary Wittert, an endocrinologist and professor of medicine at the University of Adelaide. “The drug is only effective as long as you take it.”
In two of Novo’s own clinical trials, patients taken off the treatment regained most of the weight they had lost within a year after stopping the medicine. The Danish drugmaker sells Wegovy — the first new obesity drug to reach the market in years — and another treatment for diabetes with the same key ingredient, called Ozempic. Eli Lilly & Co. has a similar diabetes treatment, Mounjaro, that’s under review for weight loss.
The medicines’ success so far puts them on track to be some of the pharma industry’s best-selling drugs, causing supply shortages and forcing Novo to ration starter doses to favor existing users over newcomers. The market for obesity alone could reach $44 billion by 2030, according to Bloomberg Intelligence.
“If you ask a person living with obesity, severe obesity, if you ask that person whether he or she feels it is a chronic disease, I think they would say this is chronic,” said Lars Fruergaard Jorgensen, Novo’s chief executive officer. He likened it to someone with hypertension seeing their blood pressure rise again if they didn’t take their medicine. “For many, if you stop treatment, you’ll just regain the weight.”
When the UK health-cost assessor issued its recommendation for capping treatment at two years in March, it said that was based on Novo’s own models, which showed that’s the longest most people are usually treated by weight specialists.
Novo, however, has long argued that treatment will last much longer. Jorgensen said some people may be able to switch to less effective or older medicines after “some time.” He suggested that others may be able to quit and keep the weight off thanks to drastic lifestyle changes “because losing weight empowered them,” though he emphasized this is a personal view. The company said at a press briefing in June that it was interested in research into how weight loss could be maintained with less medical intervention.
Balk, the Yale dietitian, started taking Ozempic last August when he was more than 30 pounds overweight. At 43, he has a family history of diabetes. He now provides nutrition advice to a fee-based online group started by an Ozempic patient for people who don’t have access to support elsewhere.
The treatment addresses only part of the problem, according to Balk, who describes an environment, especially in the US, where people are simultaneously encouraged to over-eat and stigmatized for doing so.
“We are constantly inundated by psychological messages to ‘eat this,’” he said. “You drive down the street and there’s places for food everywhere and there’s mechanically created smells that draw you,” he said. “This is why I’m so passionate about relaying to people that this is not your fault. This is not something you failed at.”
At this year’s European Congress on Obesity, some doctors warned that even asking about patients stopping treatment trivializes obesity.
“If people recognized obesity for the real disease that it is, there wouldn’t be this debate,” said Lee Kaplan, who retired from a four-decade career at Harvard Medical School and Massachusetts General Hospital last year and now works as an industry consultant and as director of The Obesity and Metabolism Institute in Boston.
Still, Kaplan allowed that many patients do want to stop. He blamed the mindset surrounding obesity, saying that even after seeing dramatic results, people believe they shouldn’t need the drug. But when they stop injecting, hunger returns and so do the patients, seeking another prescription.
“I have yet to have a patient that stopped twice,” Kaplan said.
In support groups on social media, however, people actually report doing so multiple times.
Besides finances, some can’t manage the side effects, which can include nausea, vomiting, uncontrollable bowel movements and a phenomenon known as “sulfur burps.” Others have missed weeks of treatment due to ongoing supply shortages. The long-term health impact of the drugs also remains unclear, even though Ozempic has been available since 2018.
In Kentucky, Shelly Gilbert first stopped taking Ozempic for a few weeks at a time earlier this year as shortages delayed her prescriptions. Then in April, she was switched to a new insurer, UnitedHealth Group Inc., and lost access completely.
A 45-year-old housing administrator, she had battled her body since her 20s, when she was a personal trainer and started gaining weight inexplicably. She was diagnosed with polycystic ovarian syndrome, a hormonal disorder that often causes weight gain.
“I tried all kinds of diets, of course, like a lot of people,” she says. In 2021, Gilbert followed a medical weight-loss program at a hospital for six months. She lost 10 pounds.
Frustrated at so little output for so much effort, she started taking Ozempic in October of that year and lost another 64 pounds. After her last dose in mid-March, she regained close to 30 pounds despite watching her diet and doing yoga. “I just think it’s going to keep going up,” she said. “It’s just really the way my body processes food. This type of medication is the only thing that’s been effective for me.”
The chief executive of her insurer, Andrew Witty, told investors recently that the company needs to be clear which patients benefit from the new drugs. If everyone were to be covered indefinitely, the costs would be astronomical, especially in the US, where about 42% of the adult population has obesity.
A spokeswoman for UnitedHealth acknowledged e-mails seeking comment but didn’t respond to the specifics of the case. A few days later, however, Gilbert logged into the insurer’s website and was surprised: her request for Ozempic had finally been granted.